News Articles
This site contains over 2,000 news articles, legal briefs and publications related to for-profit companies that provide correctional services. Most of the content under the "Articles" tab below is from our Prison Legal News site. PLN, a monthly print publication, has been reporting on criminal justice-related issues, including prison privatization, since 1990. If you are seeking pleadings or court rulings in lawsuits and other legal proceedings involving private prison companies, search under the "Legal Briefs" tab. For reports, audits and other publications related to the private prison industry, search using the "Publications" tab.
For any type of search, click on the magnifying glass icon to enter one or more keywords, and you can refine your search criteria using "More search options." Note that searches for "CCA" and "Corrections Corporation of America" will return different results.
Hampton County Detention Center, SC, SHP Medical Intake Forms, 2020
Document text
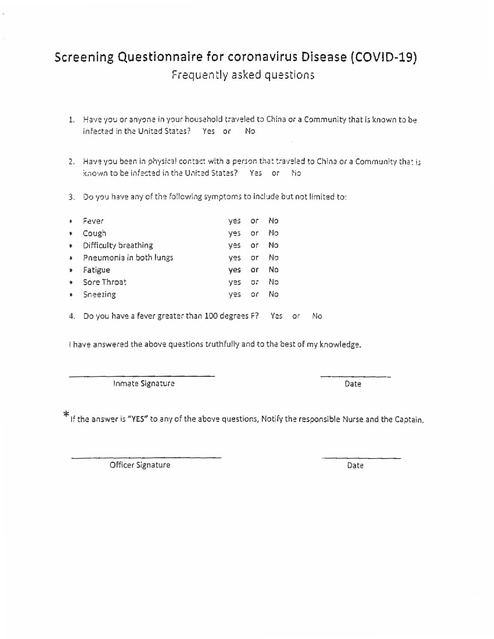
Screening Questionnaire for coronavirus Disease {COVID-19)
Frequently asked questions
1.
Have you or any-:,ne in your household t:-av:led t::i China or a Community that is known to be
infected in the United States?
Yes
or
No
2.
Ha·,~ yo1.J been in physical cont:1,:t with a person t:iat t:a•teled to China or a Community tha~ i.;
:<r1own to be infected in the U,1i:ed States?
Yes or No
3.
Do yo:J ha'!e any of the following symptoms to indude b 1.Jt not limited to:
I
Fever
yes
or
No
•
•
•
•
•
•
Cough
yo~
_.,
or
No
Difficulty breathing
yes
or
No
Pneumonia in both lungs
yes
or
No
4.
Do you have a fever greater than 100 degrees F?
Fatigue
yes
or
No
Sore Throat
yes
o:-
No
Sneezing
yes
or
No
Yes
or
Mo
I have answered the above questions truthfully and to the best of my knowledge.
Inmate Signature
Date
* If the answer is "YES" to any of the above questions, Notify the responsible Nurse and the Captain.
Officer Signature
Date
rl-\~,IPTON DETENTION CE~TER
1:--; !TI.-\L NTAKE,' TRHGE QUESTIONS
rTO BE ASKED Of TR..;.~~SPORTNG OFFtCER)
I
I
I
I
I
1. Has this person been injured or h'.l\. e any observable medical problems?
If yes, explain:
I
I2. l Has this person exhibited any mental health/suicidal behaviors?
i
If yes, explain:
i
Has this person tried to escape or acted violently?
If yes, explain:
4. Is there any other information about this individual \Vhich \Ve need to
know?
II
If yes, explaL'l:
I
Nol
Yes
I
I
I 3.
Yes No
IYes
No
Yes No
I
I
5. Ha3 a NCIC check been run?
If yes, explain:
Yes No
6. Are there any active warrants?
If yes, explain:
Yes No
Subject Name:
Transporting Officer:
Intake Officer:
Other Comments:
l
Date:
Time:
Agency:
I~ITL..\L ~lEDIC.-\.L Il'-iTAKE & HISTORY
J~
Naml:!
--------
--------------
Age___
•• 1~,'a;;
Sex- - - - - - - -
Examiner's Name:____________ Dnte________
Inmate taken to ER prior to booking·? Y or N (If yes. ckar:ince fonn must be placed in l'iur;e·, bo·q
Bookin<1 Officer's Visual O inion
I. [.; the inmate cor.JcioLJs
., Does the inmate have pain. bleeding or oth.:r symptom.5 needing Em,ergency Services?
J,
i
I
l
I
i
I
!
!
I
I
i
I
I
I
I
I
I
I
i
.
w
•
.
"
. -
:.:,
•
'
'-"
w
:,
l
l '-
w
.:,-
.
Yes or No
Yes or No
::,
Ye·orNo
'
l
I
l
Care?
I
fs t!1ere obvious f.!ver, swollen lymph nodes. jaundice or other ,evidence of infection
Yes or No I
which mav soread throum facilirv'?
5. [s the s!<in in good condition & free of vermin? (If no, explain)
Yes or No
6. Does the inmate appear to be under the influence of alcohol·?
Yes or No
7. Does the inmare appear to be under the influence or barbin1rates, heroin or any other
Yes or No
dru2?
8. Are there any visible signs of Alcohol/Drug withdrawal symptoms?
Yes or No
9. Does the inmate· s behavior suggest the risk. of suicide?
Yes or No
I 0. Does the inmate's behavior su~gest the risk of assault to staff or other inmates?
Yes or No
I I . fa the inmate carrying medication or does the inmate report being on medication which
Yes or No
should be administered or available?
Officer-Inmate Questionnaire
I
12. Are you presently ta!<lng any medication for diabetes, heart disease, seizures, arthritis,
Yes or'No
asthm1. ulcer:;, HBP. or psvchiatric disorder? (List condition)
13. Do you have a special diet prescribed by a physician? (ff so, list)
Yes or No
14. Do you hav~ a history of Communicable Di.,ease? (ex. HIV/AIDS, MRSA, TB, STD)
Yes or No
15. Have you recently been hospitalized or seen a medical or psychiatric Dr? (If so list)
Ye.s or No
Do you stiU feel suicidal?
l 6. Have attempted suicide? [f so, when?Yes or No
17. Are you allergic to any medications, foods, plants, or fabrics? (If so, list)
Yes or No
18. Have you fainted recently or had a recent head injury? (lf so, when?)
Yes or No
19. Do you have Epilepsy, history of TB, Diabetes, or Hepatitis? (ff so list)
Yes or No
20. Females: Are you pregnant? How many months?
Yes or No
21. Females: Are you on birth control?
Yes or No
22. Females: Have you recently given birth'? How long ago?
Yes or No
_.}.
Do you have a painful dental condition?
Yes or No
2-k Do you have a complaint of sore throat. fever, or any condition that may spread?
Yes or No
..,_:::,,
- Do you have any other medical conditions or problems we should know about?
I Yes or No
List any medicat10ns hvI 1s presently taking__________________
Any History of Narcotic Use? YorN____________________
...
. ,~
Dietary Preferences? ___________________________
I agree that the above infonnation can be released to an1 counselor or attending physician
Inmate Signature
Officer's Signature
PATIENT'S CONSENT FOR TREATMK'iT
The undersigned, being in the custody of the County Jail, hereby authorize and request that all
medi~al record.5 and/or information, . .vher-ever located, including anv ho:mitc1ls
or medical doctor
.
or any other place where medical record.5 may be located, be released to the County h.il medical
department for use by the medical department regarding any treatment to be reviev,,ed while in
custody. I undentand I ""ill provide this information to the medical department.
-
;
I further authorize the County Jail medical department to evaluate and treat any condition that I
may have or develop while in the custody of the County Jail. My signature below hereby
authorizes other healthcare providers to provide medical infonnation regarding my medical
condition to the staff of Southern Health Partners while in the custody of the County Jail. This
care may result in services being provided outside the County facility which may include but not
be limited to hospitais, clinics and physicians' offices. Furthermore, my signamre belo\.v
provides consent for medical photographs to be made for me. I understand that the photographs
and informaiion may be used in my medical record for the purposes of documentation and/or
treatment. I ad~no\1,fodge no guarantee or a.5surance ha3 been made as to the desired result that
may be obtained.
I have been made aware of how to request medical services while incarcerated, and am a·ware I
have the right to refuse treatment. I may be required to sign a Refusal of Treatment fonn should
I refuse medical treatments and/or medications.
I release Southern Health Partners, Inc., its staff, the County, the Sheriff (where applicable),
his/her staff from all responsibility and I assume personal responsibility for the conditions that
may occur as a result of my not requesting services and/or refusing treatment as prescribed by
the medical staff of the facility and/or outside consultation services.
Patient's Signature: __________________
Date: - - - -
Printed Name: -------------------- Patient's DOB: ----Witness: _____________________ (Officer/Medical Signature)
,; Jt-t.
r:11:; :,J1npl,ndform mr,;t bfl grvttn tfJ the m,:du:al deparnn,mr f or i11c/11:;ifJn m the pati,mt ·_. cfJnjld,m11al mctdrcal fr!tt
'J/thi; ffJ1'nr 11pr,11 ,·-1qr,e;t. ifpm1l!t11 rs 1ra11~'f"'rt-tdiJr 0111: 1dt! m.trlical :;l!rv,ce.;
SHP Form 11'06, Vpda1.:d Januar:1 20 15
P!~au prfJ,•ufe a ;l)py